ARRS Case of the Week
CHEST IMAGING
Case Author: Christopher M. Walker, MD, Saint Luke’s Hospital of Kansas City, University of Missouri–Kansas City
History
54-year-old patient with long-standing dyspnea and cough.
Findings
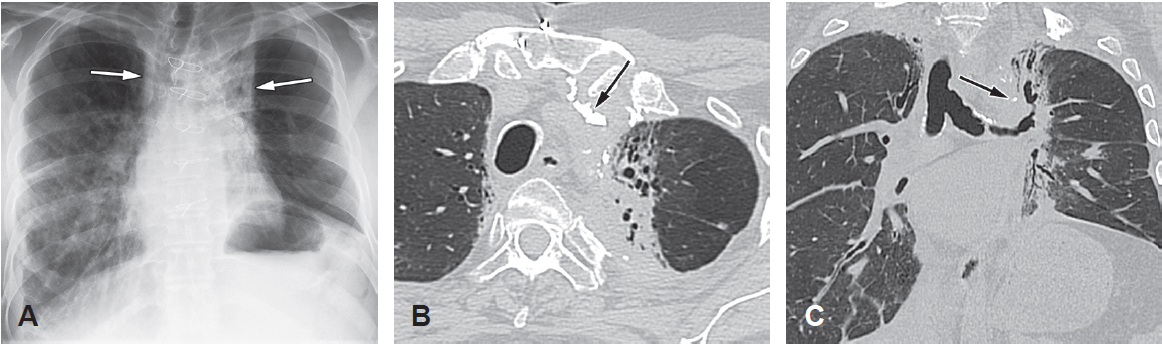
Posteroanterior chest radiograph (A) shows reticular opacities predominant in the mid and upper lung zones with features of volume loss. Axial (B) and coronal (C) contrast-enhanced CT images show patchy bilateral ground-glass opacities, reticulation, architectural distortion, and traction bronchiolectasis (black arrow, B). Extensive mosaic attenuation with hyperlucent portions of lung is caused by air trapping (white arrows).
Differential Diagnosis
- Hypersensitivity pneumonitis
- Organizing pneumonia
- Respiratory bronchiolitis–interstitial lung disease
- Sarcoidosis
Correct Diagnosis: Hypersensitivity pneumonitis
Most patients (80–95%) with hypersensitivity pneumonitis are nonsmokers.
CT features that favor a diagnosis of hypersensitivity pneumonitis over other fibrotic lung diseases include mosaic attenuation, predominance in the mid or upper lung zones, and centrilobular ground-glass nodules.
Bronchoalveolar lavage in patients with hypersensitivity pneumonitis generally shows an increased number of WBCs, of which 20–30% are lymphocytes. The T-cell CD4:CD8 ratio is often less than 1, whereas the CD4:CD8 ratio in sarcoidosis is often elevated to more than 3.5.
Hypersensitivity pneumonitis is treated by withdrawing exposure to the causative agent. Corticosteroid therapy may be helpful in alleviating acute symptoms.
Suggested Readings
Choi YW, Munden RF, Erasmus JJ, et al. Effects of radiation therapy on the lung: radiologic appearances and differential diagnosis. RadioGraphics 2004; 24:985–997
Park KJ, Chung JY, Chun MS, Suh JH. Radiation-induced lung disease and the impact of radiation methods on imaging features. RadioGraphics 2000; 20:83–98